
The AARC Program
The Alberta Adolescent Recovery Centre is a long-term program backed by research, specializing in treatment for youth and young adults aged 12 to 21 who struggle with alcohol/drug use.

"At AARC, I've witnessed the incredible strength of youth and their families as they overcome addiction together - there is no other program like it - and AARC staff are here to walk through that journey with them every step of the way."
Donny Serink, BCC, MSW, RSW
Executive Director


Are you struggling with your teen?
Speak with an expert adolescent addiction advisor today. We’ll listen with empathy, care, and complete confidentiality.
AARC’s Unique Treatment Model
Our 12-step clinical-based treatment model with psychiatric, psychological and social support.
Treatment for the Entire Family
AARC understands that the youth addiction journey can impact parents, siblings, and extended family members. A cornerstone of the AARC program is that we provide support for family members participating in treatment. We work together to rebuild youth and reunite families.
Family commitment plays an integral part in the success of the AARC treatment model. As your child advances through the four levels of treatment, family members also receive personalized support for the duration of treatment. This individualized care focuses on supporting the family members themselves, offering them the tools and guidance needed to cope with challenges and navigate the road ahead.

Affordability
At AARC we believe every child deserves the opportunity to step into living a substance-free life. Thanks to the generosity of our loyal donors, partial funding from the Government of Alberta, Ministry of Mental Health & Addiction, and community events, access to treatment is based on need and fees are based on ability to pay. We assess individual fees based on each family’s unique financial situation, ensuring families only pay what they can afford. No one requiring AARC’s intensive program is turned away based on their inability to cover the costs.

AARC’s Specialized Clinical Team
AARC’s multidisciplinary team consists of a diverse group of professionals in areas including Psychiatry, Social Work, Canadian Addictions Counselling, Nursing, and Youth Peer Counselling. AARC recognizes that addiction is a complex Biological-Psychological-Social-Spiritual interaction and, therefore encompasses all of these approaches within our unique treatment model, designed to also support concurrent mental health disorders.

Peer Counselling
Beginning this journey can be overwhelming. In addition to our team of medical and mental health professionals, each client is provided with a mentor from our Peer Support Team. The AARC Peer Support Team is composed of young adults with lived experience, successfully living in sobriety, many of whom are graduates of the AARC program themselves. Their compassionate approach and encouragement provide a unique connection to support clients. This relatability is key for youth who are entering treatment feeling hopeless and alone. As we say at AARC, they are Hope in Human Form.
“At AARC, they didn’t just treat his addiction, they helped us rebuild our family. They gave my son something no other short-term program could – time. Time to recovery with dignity, which is something I believe everyone deserves. Over the course of 8-10 months, he was given the space to face his pain and begin healing, free from the substances that had taken over his life.”
AARC Graduate Mom
Long-Term Treatment
While the average time spent in treatment is 8-10 months, completing the program is not time limited as we recognize that each family’s journey is unique.
Abstinence-Based 12-Step Program
The treatment model at AARC is based on the 12-Steps of Alcoholics Anonymous. For youth, this is broken down into 4 comprehensive levels, leading to total abstinence. At AARC, we recognize that drug and alcohol addiction is a chronic disease requiring lifelong recovery.
Treatment at AARC is delivered through intensive individual and group counselling sessions held multiple times per day. These sessions are facilitated by an exceptional team of Youth Addiction Specialists, including Social Workers, Certified Addictions Counsellors, Clinical Counsellors, and members of our unique Peer Support Team, many of whom are graduates of the AARC program themselves, successfully living in sobriety. As they are supported through this therapeutic work, youth are encouraged to recognize and acknowledge the reasons behind their harmful drug and alcohol use, despite the negative consequences. They develop tools to navigate a successful and productive life substance-free.
Overall, the primary focus of the AARC program is to help struggling youth identify their unhealthy/high-risk patterns, develop coping skills, restore family relationships, reintegrate into school or work, and prepare for sustained sobriety post-treatment.
Post-Treatment Support
After graduation, youth and their family members can continue to access the services offered by AARC and are encouraged to stay connected to their community, with opportunities to give back by helping new families in treatment.
As part of this ongoing network, AARC community members often remain involved after formal treatment ends, offering guidance to new families as they navigate their journey. Emphasis is placed on sharing experience, strength, and hope, with a deep understanding of the challenges, based on their own lived experiences. This provides a space for vulnerable conversations and building supportive connections. The AARC community comes together in unity, providing a powerful source of strength and ensuring that no family faces their journey alone.

Nutrition & Fitness
As part of the focus on nutritional health, the AARC facility includes a full kitchen with chefs providing nutritious and well-balanced meals throughout each day. There is also a strong focus on physical health where clients work with a Personal Trainer 3 times a week in the AARC fitness center. Clients also have access to an Activity Room, Outdoor Hockey Arena, Basketball Courts and other amenities to keep their minds and bodies active during treatment.
AARC’s Unique Recovery Homes:
Semi-Residential Treatment
One of the unique strengths of AARC’s model is its semi-residential component. While the youth spend their days at the Centre, they do not spend their nights within the facility. Instead, they go to the homes of other families further advanced in the program. This therapeutic component is a critical part of the healing process for families and youths and provides a community of support during treatment and post-graduation.
For new families in treatment, this provides much-needed respite and time to heal. For your child, the experience is less institutionalized because they go to a comfortable and caring home after an intense day of therapy. For host families, it provides the opportunity to support other youth in sobriety and learn how to rebuild the family structure after the chaos of addiction.
AARC’s Recovery Homes are private residences accredited by the Canadian Accreditation Council of Human Services. AARC provides extensive training and guidelines for operating a home and provides 24/7 on-call support.
“Recovery homes are an amazing component of the AARC treatment model. When it came time for us to open our host home, AARC provided us with thorough training and checked our house with the utmost care to ensure safety for all …. Our daughter was trained as a host home oldcomer so she could provide leadership with the newcomer … Not only did this provide our daughter with an opportunity to take responsibility, regain healthy boundaries, and give back to other young people, it once again modeled to new clients that there is a way out of the disease of addiction."
AARC Graduate Mom
Research-Based Treatment Program
-
Effective Approaches to Adolescent Addiction: Evaluation of the Alberta Adolescent Recovery Centre (AARC) Findings and Implications for Clinicians, Researchers, and Policymakers
In 2015, AARC was awarded a $300,000 grant to fund independent research on the efficacy of their program. Independent researchers conducted retrospective interviews with a sample of program participants. They assessed the impact of the AARC program on standard measures of drug abstinence, psychosocial and academic functioning, and overall health. The Principal Investigator on the evaluation was Dr. Amelia M. Arria, Ph.D, University of Maryland and the Co-Principal Investigator was Dr. Ken C. Winters, Ph.D., University of Minnesota.
The research emphasized the importance of offering thorough care that addresses the needs of both individuals and their families. It also highlighted the necessity of recognizing the distinctive developmental requirements of adolescents and the significance of understanding the social context and other environmental factors that can affect the success of the program.
Research Highlights
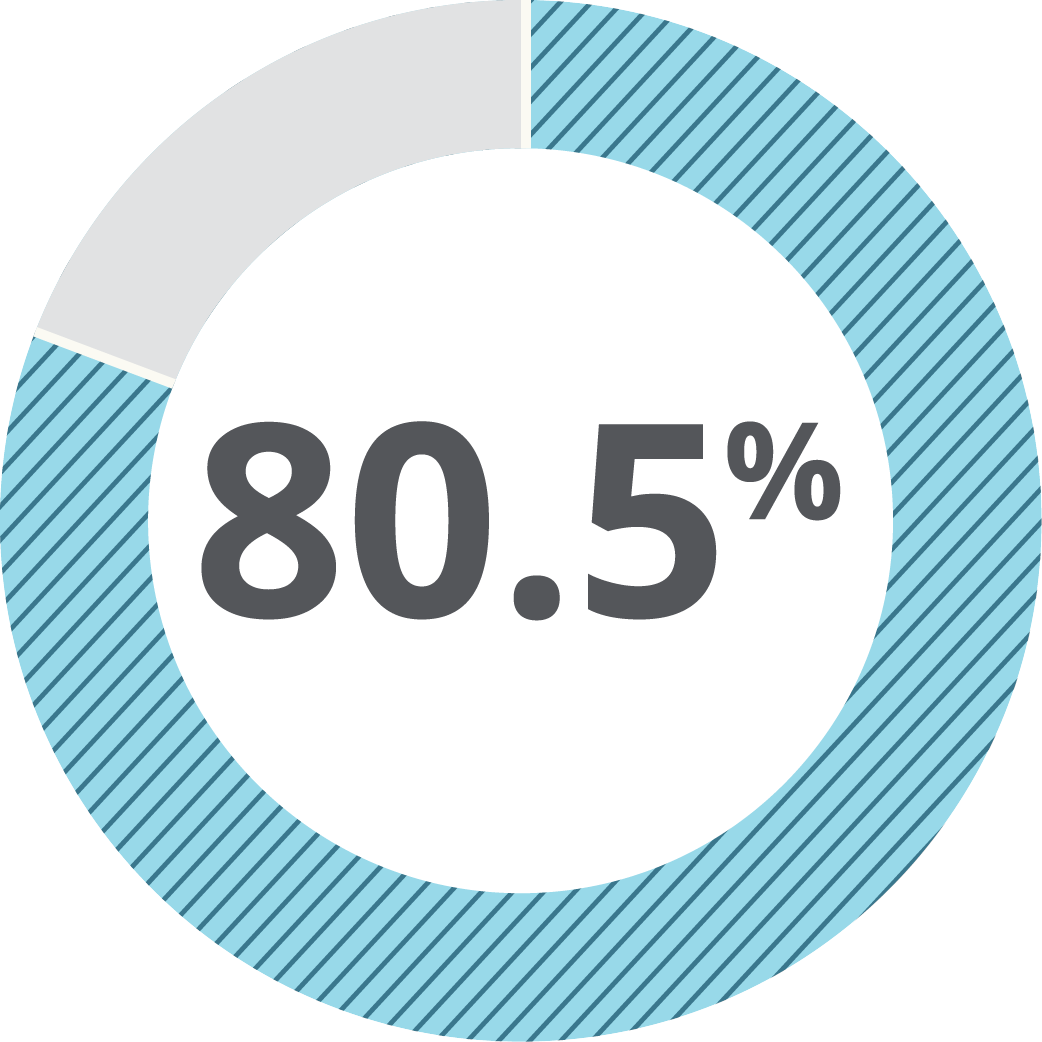
of clients who entered treatment at AARC completed the program
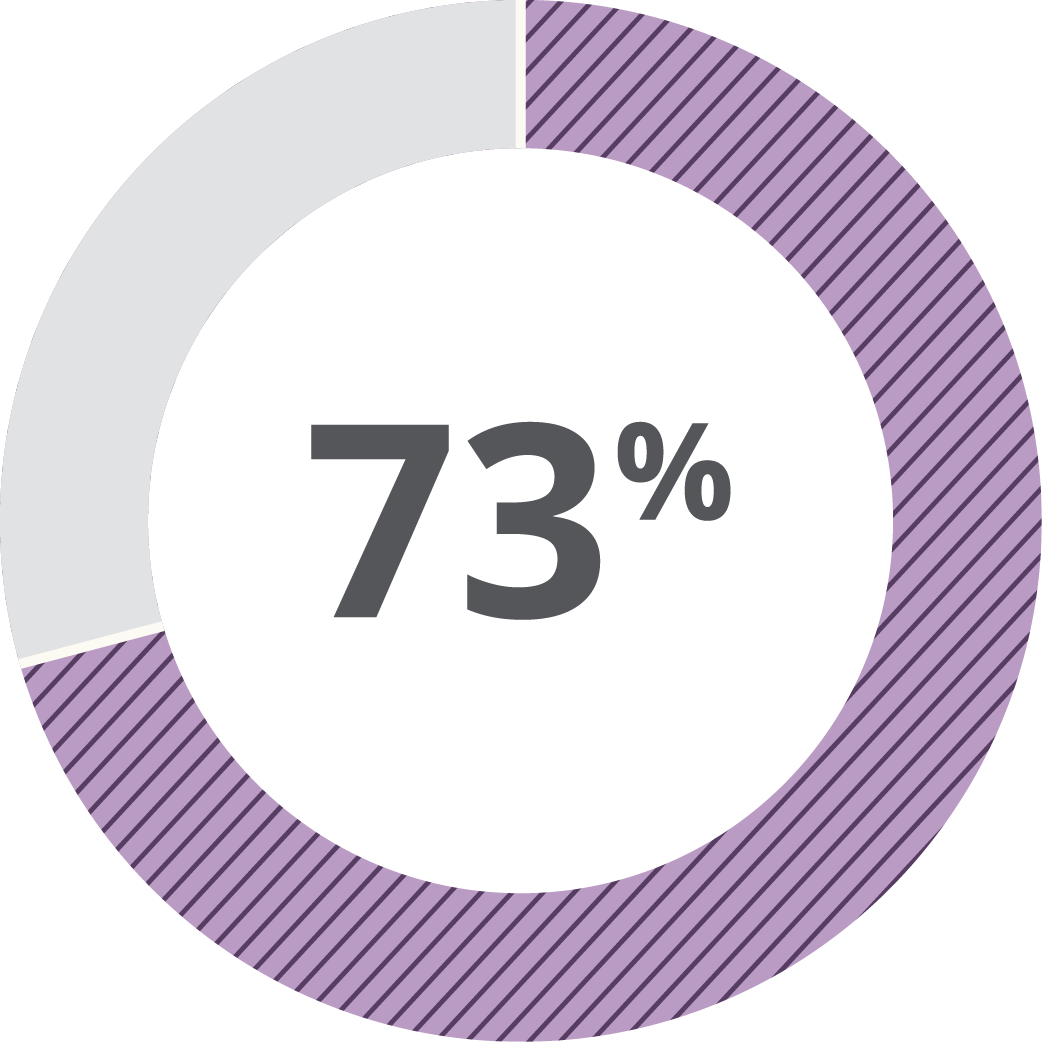
of AARC graduates reported remaining abstinent from drugs & alcohol 12 months after graduation
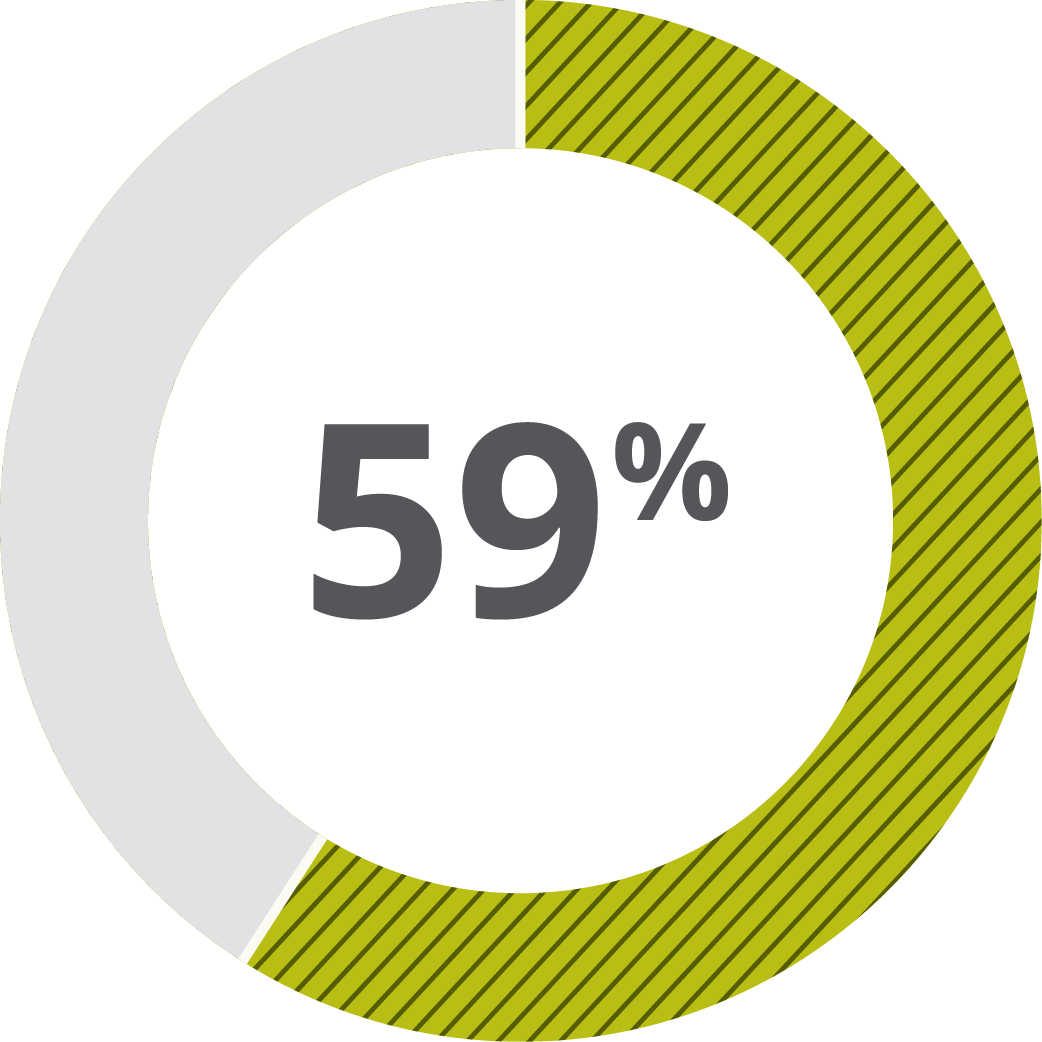
of AARC graduates reported remaining abstinent from drugs & alcohol 24 months after graduation
“AARC provides an impressive model of a long-term comprehensive, semi-residential treatment program. In the context of the published outcome literature, the proportion of AARC graduates who were abstinent from drug use is impressive.”
Dr. Amelia Arria, University of Maryland
Director, Centre Young Adult Health & Development
AARC provides an integrated approach to healing by addressing the mental, physical, and spiritual aspects of recovery.
“For years, we watched addiction change my son into someone we didn't recognize. The AARC program not only saved his life but supported our family when we felt totally hopeless. It is truly a miracle that our son is alive and living a sober healthy life. We’re forever grateful.”
AARC Graduate Mom